I thought I would talk today about what we have used our simulation suites for so far. As I mentioned in my last posting, a simulation suite is composed of one room containing the simulator separated from a control/debrief room by a one-way mirror.

I know that many of you use simulation in your programs. For example, parents and students are simulated in the faculty of Education; clients and families are simulated in Social Work just to name a few. In nursing, we have always simulated patients, clients and families. These suites give us the ability to simulate psychomotor skills with a high degree of fidelity to the human experience, but also to get at some of the more nebulous parts of nursing like communication, teamwork, delegation and conflict management.
So far, we have had first year BSN students in the suites learning the fundamental skill of taking vital signs, and 4th year BSN students reenacting a critical incident (anaphylaxis). In the critical incident, the sessions were videotaped and there was a debriefing after. The debriefing is meant to be more than just another opportunity for being the ‘sage on the stage’ and teaching; it is meant for critical reflection and deep learning about ways of thinking and knowing, and about the assumptions held that lead to the actions taken. I will be writing more specifically about debriefing in later blogs, so I will not go into any great detail here, but the importance of debriefing cannot be overemphasized.
With the 2nd year BSN students, I took a slightly different tact. Due to room size issues, our typical class of 72 is split into two cohorts for theory classes. This year I was teaching both cohorts of the 2nd year relational practice (read communication) course. I asked for a volunteer from each class to do a simulation with me that we would debrief with the entire class. Two brave souls came forward, and I set up the simulation lab to best capture an interaction between the student and a simulated patient. I asked a local actor (okay, he’s my partner) to play a man who was about to be discharged from hospital, but just before he goes, he gets bad news from the physician. The only information the students had was that they were going in to do a last quick assessment on him before he was discharged. I told them to do a set of vital signs and get him ready for discharge, but mostly to concentrate on forming, then terminating, a therapeutic relationship. As they were doing their assessments and getting to know him, I came in as the physician, delivered the bad news, then left.
The point I was trying to make with this simulation is that in times of stress, we all revert to what is safe and comfortable for us in our communication. For a novice nurse being with a patient when he gets bad news then being alone with him after would certainly be a stressful situation. This simulation was intended to help them notice what their ‘safe’ pattern or habit was, and for their peers to think about their own patterns of communication and what their ‘safe’ pattern might be.
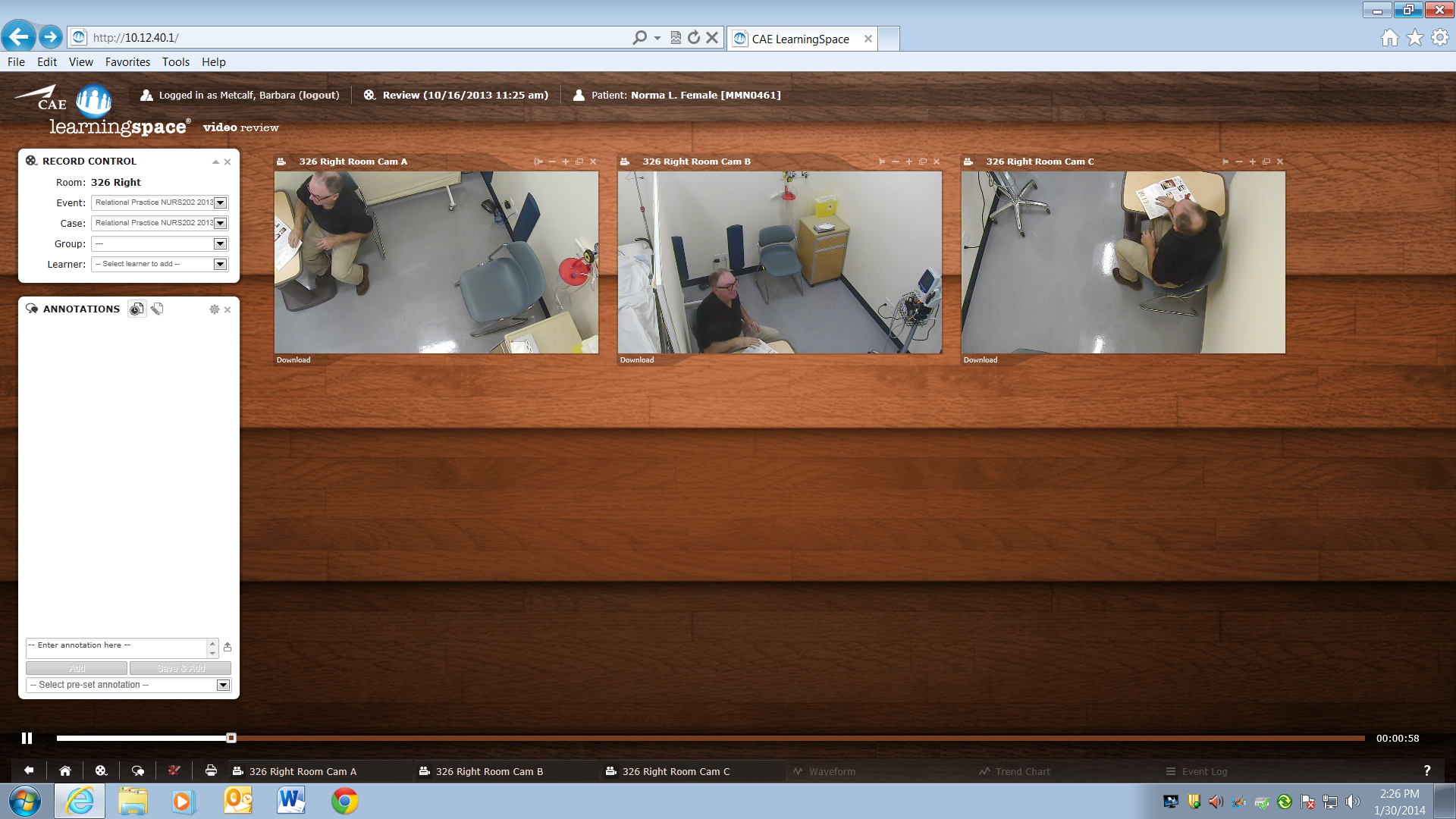
We were very lucky in our choice for the simulation learning management system because the tapes of our simulations are actually housed on the web. This means that we can replay these taped sessions on any computer on campus. I was able to play the sessions back in the big classroom (although we had sound issues and ended up having to all go down to the sim suites anyway) so that everyone could see the playback together. The simulations could not have gone better, and what was terrific was that each student had a different ‘safe place’ for communication. Both agreed to allow me to show their simulation to each class, so we could see first-hand how each person may have a different pattern or habit s/he may fall into. The students were also able to talk about their discomfort with the situation and how powerful the experience was when doing this with a real person. Normally, I would simply have approached this topic by asking students if they have identified any of their own habits of communication in clinical practice. The only down side to this simulation was with camera placement. All three cameras in each room are ceiling mounted, so as you can see by the picture above, we could not get people’s faces to any great degree. 20/20 hindsight. Despite this, the combination of simulation with the ability to tape and playback was quite powerful and allowed me an almost tangible way to move into a discussion about something of which most students are unaware.
I hope that some of you will share some of the ways you have used simulation in your courses. I will outline my future plans for the suites in a future blog. Cheers and until then. Barbara